We spoke to Prof. Hamady to learn more about his lecture at CIRSE 2022.
Stent conformability and apposition influence long-term durability and remodelling
Watch this lecture in the session “What is happening in the aortic arch?“
Aortic arch pathology frequently presents a range of anatomical challenges including angulation, tortuosity, non-uniformity of the landing zone as well as short length. Despite promising early clinical results, the older generations of thoracic aortic stent grafts are known for their inherent stiffness and sometimes cumbersome deployment mechanisms.
Poor opposition of the stent graft with the aortic wall is associated with an increased risk of endoleak and graft migration. The observation of bird beak configuration (BBC), defined as the non-alignment of the lower edge of the stent against the inner curve of the arch, has been reported to increase the risk of Type 1 endoleak. The formation of bird-beaking and inappropriate oversizing are also blamed for stent collapse reported in some older generation grafts.
The length and angle of BBC are proportional to the incidence of Type 1 endoleak. Dake et al. reported a 50% risk of endoleak at a bird-beak length of 9.5mm and an 80% risk at a bird-beak length of 14 mm [1]. The presence of BBC has also been linked to endoleak and remodelling of type B aortic dissection [2]. The zonal anatomy can influence the stent alignment. In a study of 164 patients, BBC and endoleak were observed more in zone 1 and 2 when compared with zone 0 [3].
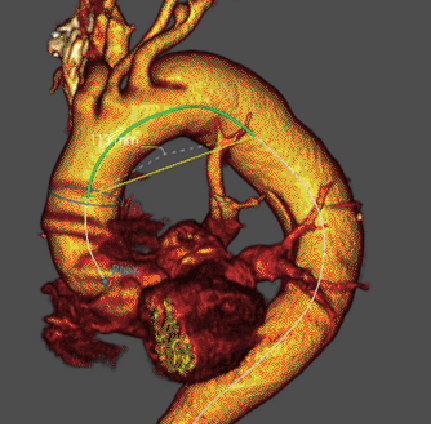
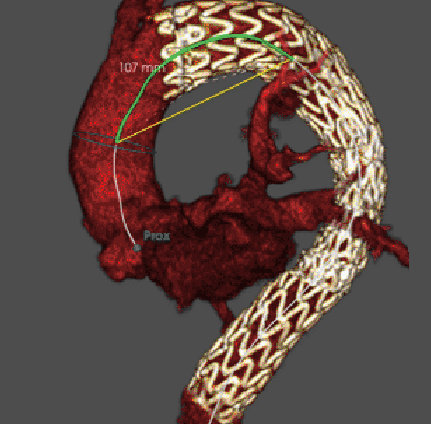
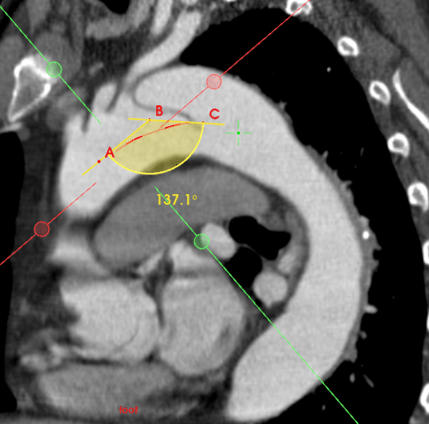
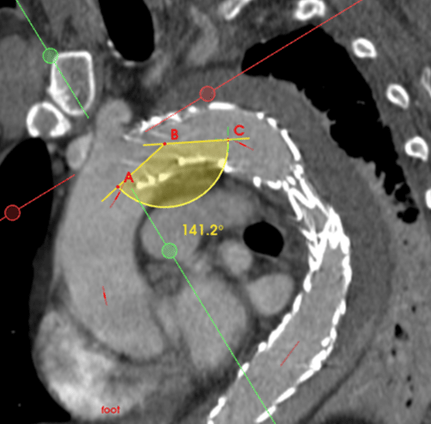
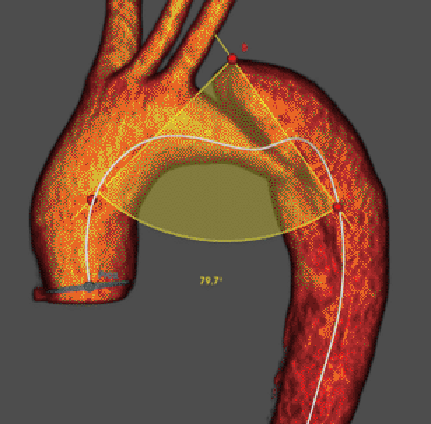
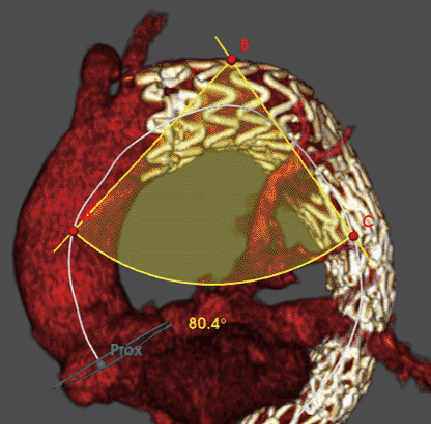
The new developments in stent technology have addressed the issues of stiffness and conformability to various degrees [4]. The performance of conformable TAG stent graft (Gore Medical, Flagstaff, AZ, USA) is assessed in 58 consecutive patients with a median age of 75 and a range of aortic pathology including degenerative aneurysms, dissection, penetrating aortic ulcers, and intramural haematoma. One third of patients are treated in an emergent setting. The technical success rate of the index procedure is 98%. One Type 1 endoleak is detected and treated with stent extension. The interesting finding is that arch angulation, arch width and landing zone angulation have not significantly changed pre and post-procedure despite stent landing in type III arch in more than two-thirds of cases (figures). Two cases of bird beaking configuration are noted with no associated endoleak nor stent collapse. Both BBC cases are noted in zone 2 and in type III arch. (paper under review for publication).
The use of Conformable TAG with Active Control (Gore Medical, Flagstaff, AZ, USA) has been reported in a retrospective series of 30 consecutive patients. The indications are post-dissection aneurysms, degenerative aneurysms, IMH, and traumatic aortic injuries with 63% of patients being treated in elective settings and the rest in emergent ones. Besides the high technical and clinical success rate, there is no BBC nor Type 1 endoleak noticed in this cohort of patients. The authors report the use of active control for optimisation of alignment in all cases [5].
Similar results are observed in the SURPASS registry. 127 patients are included in this registry to treat a range of aortic diseases. The technical success is achieved in all cases. Active control to optimise wall opposition of the stent graft to the inner curvature of the aortic arch is reported in 60% of patients and the desired effect is achieved in all cases. No BBC or migration is noted in this series [6].
Other manufacturers have also made changes to the design of respective stent grafts. A series of 38 patients with challenging arch anatomy including short landing zone and increased arch and landing zone angulation are treated with custom-made scallop Relay (Terumo Aortic, Sunrise, Fla). Technical success is reported in 98% and non-disabling strokes occurred in 8%. At a median of 4.5 years, all-cause and aorta-related survival rates are 72% and 85%, respectively. Freedom from reintervention to the thoracic aorta and PLZ is 92% and 97%, respectively. The BBC is observed in approximately 28% of this cohort, despite the extreme adverse anatomical features in the enrolled subjects including a very short landing zone prior to stent insertion (median 5mm) (median sealing zone post scallop insertion of 26mm). Two-thirds of patients have acute angulation with type II and III arch. The mid and long-term follow-up show no type I endoleak or evidence of 5 mm or more migration [7].
Similarly, Valiant Captiva and Valiant Navion stent grafts (Medtronic, Santa Rosa, CA) have reported encouraging results regarding technical success and low incidence of Type 1 endoleak and very low migration. Unfortunately, Valiant Navion has been withdrawn from the market because of reported stent fractures. There has been no comprehensive study to assess the conformability and incidence of bird beaking related to this stent type [8,9].
Future directions should focus on an in-depth understanding of aortic movement during the cardiac cycle as well as physiological flow characteristics and their impact on stent graft long-term durability. Refining stent cloth material and the skeleton to adapt to the physiological changes post stent implantation should be properly appraised. Platforms with a lower profile and delivery systems with accurate deployment mechanisms should also continue to evolve [10-12].

Mohamad Hamady
Imperial College, London/UK
Professor Hamady completed his clinical training in interventional radiology at King’s College-London/ St Thomas’ & Guys hospitals. He joined the Imperial College NHS Trust in 2003 as a consultant in clinical and interventional radiology. He is currently Professor of Practice in Image Guided Surgery and Interventional Radiology at Imperial College London.
Professor Hamady is a world-renowned expert on aortic and peripheral vascular interventions and advanced embolisation techniques. He has done extensive research work in complex endovascular aortic repair, simulation training and endovascular robotics. He has more than 185 papers in peer-review journals and 16 book chapters. He has served in several positions within the British Society of Interventional Radiology (BSIR), including as the Chair of the Scientific and Education Committees, and as the Society’s Secretary. Currently, Professor Hamady is the BSIR Council Lead for IR Workforce in the UK, the Head of Training Program for Interventional Radiology in Greater London and the Chair of the Scientific Committee of IDEAS/CIRSE 2020-2022.
References
- Ueda, T., Fleischmann, D., Dake, M. D., Rubin, G. D., & Sze, D. Y. (2010). Incomplete endograft apposition to the aortic arch: bird-beak configuration increases risk of endoleak formation after thoracic endovascular aortic repair. Radiology, 255(2), 645–652.
- Cao L, Ge Y, He Y, Wang X, Rong D, Lu W, Liu X, Guo W. Association between aortic arch angulation and bird-beak configuration after thoracic aortic stent graft repair of type B aortic dissection. Interact Cardiovasc Thorac Surg. 2020 Nov 1;31(5):688-696.
- Kudo T, Kuratani T, Shimamura K, Sawa Y. Determining the Optimal Proximal Landing Zone for TEVAR in the Aortic Arch: Comparing the Occurrence of the Bird-Beak Phenomenon in Zone 0 vs Zones 1 and 2. J Endovasc Ther. 2020 Jun;27(3):368-376.
- Canaud L, Cathala P, Joyeux F, Branchereau P, Marty-Ané C, Alric P. Improvement in conformability of the latest generation of thoracic stent grafts. J Vasc Surg. 2013 Apr;57(4):1084-9
- Mariani C, van der Weijde E, Smith T, Smeenk HG, Vos JA, Heijmen RH. The GORE TAG conformable thoracic stent graft with the new ACTIVE CONTROL deployment system. J Vasc Surg. 2019 Aug;70(2):432-437.
- Torsello GF, Argyriou A, Stavroulakis K, Bosiers MJ, Austermann M, Torsello GB; SURPASS Registry Collaborators. One-Year Results From the SURPASS Observational Registry of the CTAG Stent-Graft With the Active Control System. J Endovasc Ther. 2020 Jun;27(3):421-427.
- Hanna L, Abdullah A, Kashef E, Riga C, Jenkins M, Bicknell C, Gibbs R, Hamady M. Four-year results of the Bolton relay proximal scallop endograft in the management of thoracic and thoracoabdominal aortic pathology with unfavorable proximal landing zone. J Vasc Surg. 2021 Nov;74(5):1447-1455.
- Verzini F, Desai N, Arko FR 3rd, Panneton JM, Thaveau F, Dagenais F, Guo J, Azizzadeh A. Clinical trial outcomes and thoracic aortic morphometry after one year with the Valiant Navion stent graft system. J Vasc Surg. 2021 Aug;74(2):569-578.e3.
- Conrad MF, Tuchek J, Freezor R, Bavaria J, White R, Fairman R. Results of the VALOR II trial of the Medtronic Valiant Thoracic Stent Graft. J Vasc Surg. 2017 Aug;66(2):335-342.
- van Bakel TMJ, Arthurs CJ, Nauta FJH, Eagle KA, van Herwaarden JA, Moll FL, Trimarchi S, Patel HJ, Figueroa CA. Cardiac remodelling following thoracic endovascular aortic repair for descending aortic aneurysms. Eur J Cardiothorac Surg. 2019 Jun 1;55(6):1061-1070.
- Dobson G, Flewitt J, Tyberg JV, Moore R, Karamanoglu M. Endografting of the descending thoracic aorta increases ascending aortic input impedance and attenuates pressure transmission in dogs. Eur J Vasc Endovasc Surg. 2006 Aug;32(2):129-35.
- Sengupta S, Hamady M, Xu XY. Haemodynamic Analysis of Branched Endografts for Complex Aortic Arch Repair. Bioengineering (Basel). 2022 Jan 18;9(2):45.