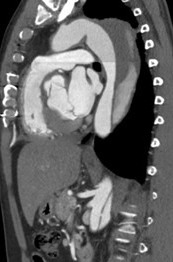
For patients with chronic uncomplicated type B dissection (TBAD), medical therapy is the treatment of choice to prevent aortic expansion, rupture and/or recurrent dissection. Blood pressure control can reduce re-dissection by two thirds. Despite appropriate medical therapy, approximately 20–40% of patients in the long-term outcome will require a secondary operation for aortic aneurysmal degeneration [1,2].
The most common indication of aortic repair in chronic TBAD is the development of chronic post dissection aneurysm of the thoracic or thoraco-abdominal aorta. An aortic diameter ≥6.0 cm should be considered for repair, taking into account patient fitness and aneurysm anatomy. The goal of the repair is to prevent aortic rupture. Other situations that may indicate aortic repair include recurrent symptoms, rapid enlargement of the aortic diameter (≥10mm/year), and clinical and imaging signs of end organ malperfusion [3].
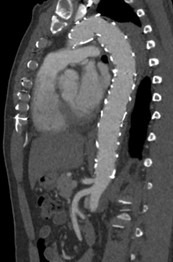
For chronic TBAD patients, conventional open surgery is currently reserved for patients with anatomy unsuitable for endovascular treatment or patients scheduled for hybrid repair due to inadequate stent graft landing zones. Over the last decade, thoracic endovascular aortic repair (TEVAR) emerged as a safe and valid alternative to conventional open surgery and has established as the preferred strategy for the treatment of the disease of the descending thoracic aorta in chronic complicated TBAD [3]. TEVAR in chronic TBAD differs from acute type B pathology based on increased stiffness of the dissecting lamella and a continued false lumen (FL) expansion. Stent-graft deployment in chronic dissection does not necessarily focus on the expansion of true lumen (TL), but aims to depressurize the false lumen by promoting progressive thrombosis. Complete thrombosis of the FL results in positive remodeling of the aorta but is only achieved in approximately 40% of patients with TEVAR alone [4,5]. Continued FL perfusion is an independent predictor of poor long-term survival and risk of reoperation or rupture [6,7].
Endovascular techniques to promote false lumen thrombosis will be discusses during the presentation. Key techniques include the false lumen occluders (FLO), Knickerbocker, “cork in the bottleneck“, and direct embolization, often applied after TEVAR (Thoracic Endovascular Aortic Repair) to seal distal re-entry tears. Although there are series of these techniques to treat patients with complicated chronic TBAD with favorable remodeling during midterm follow, available clinic reports are limited to a high-volume centres [8].
Early results of recent study show the feasibility and safety of FLOs when implanted into the FL of the infrarenal abdominal aorta [9]. The use of FLO at abdominal level offers the opportunity of one more step in a staged approach to exclude extensive aortic disease and potentially reducing the risk of SCI.
In conclusion, lifelong care for chronic aortic dissection often requires multiple staged segmental repairs. TEVAR and complex thoracoabdominal stent grafting to cover entry tears and replace aneurysmal segments of the aorta can be augmented with the adjuncts of balloon expansion of the stent graft devices and fracture of the dissection flap and embolization of the FL to promote positive aortic remodeling.