Mechanical thrombectomy (MT) has become the gold standard for patients with large vessel occlusions (LVOs), offering significantly higher rates of recanalization and improved functional independence. As technical success of endovascular procedures continues to evolve, the primary challenge has migrated from the angio-suite to the pre-procedural pathway. In the hyperacute phase, the „time is brain “paradigm remains absolute, as every minute of delay results in substantial neuronal loss. Consequently, the clinical focus is now increasingly directed toward the implementation of advanced technologies to optimise triage and patients selection.
Modern stroke management is undergoing a significant transformation through the integration of digital technologies into diagnostic and therapeutic clinical pathways.
The most profound impact of Artificial Intelligence (AI) within the hyper-acute setting is the transition from sequential to a parallel processing model. Traditional triage requires a patient to undergo neuroimaging, followed by radiological reporting and subsequent activation of the intervention team. AI-integrated platforms restructure this process by processing datasets in real-time via advanced deep learning algorithms. These systems identify LVOs and intracranial haemorrhages within minutes of acquisition, triggering simultaneous priority notifications to the entire neuro-interventional team. This allows the angio-suite to be prepared whilst the patient is still in transit from the scanner, effectively minimising the „door-to-puncture“ (DTP) timeline by an average of twenty-two to thirty–one minutes.
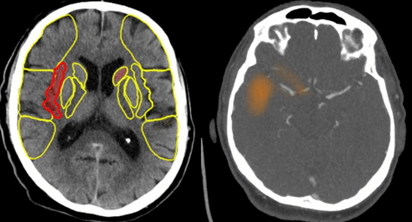
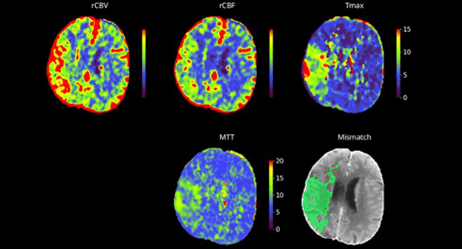
Beyond temporal efficiency, AI provides objective decision support that is pivotal for the interventionalist, particularly with automated perfusion assessment in extended time windows. By automating the Alberta Stroke Programme Early CT Score (ASPECTS) and quantifying the ischaemic core versus the viable penumbra, AI enables a more precise evaluation of tissue viability. Furthermore, in regional „hub and spoke “networks, AI implementation has been shown to reduce inter-hospital transfer delays by up to fifty per cent. Immediate image transparency allows the interventional team at the comprehensive centre to make definitive decisions instantly via mobile devices, bypassing additional diagnostic steps at the spoke site.
In conclusion, the integration of AI into the interventional workflow represents a major advancement in modern stroke management. The algorithmic prioritisation of time-critical pathologies within high-volume diagnostic datasets supports more rapid clinical intervention. Such improvements in procedural efficiency may be associated with higher likelihood of favourable outcomes for the patient’s population. Ultimately, while AI serves as an effective decision tool for triage, the final clinical determination and the performance of the procedure remain subject to clinical judgment.