Traumatic injuries to the liver and kidneys are among the most common manifestations of abdominal trauma, particularly following blunt mechanisms such as motor vehicle accidents and falls, especially in anticoagulated individuals. Over the past two decades, management strategies have undergone a paradigm shift—from predominantly surgical approaches to a more nuanced, multidisciplinary model emphasizing non-operative management (NOM) and image-guided interventions.
Liver Trauma
The liver is the most frequently injured solid organ in abdominal trauma due to its size and vascularity. Injuries range from minor capsular tears to complex parenchymal disruptions with major vascular involvement. The American Association for the Surgery of Trauma (AAST) grading system remains a cornerstone for classification, but clinical decision-making is increasingly driven by hemodynamic status rather than grade alone.
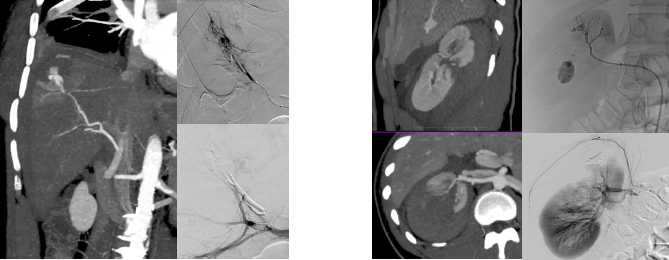
In hemodynamically stable patients, NOM is now widely accepted, with success rates exceeding 85–90%. Multiphase-contrast-enhanced CT plays a pivotal role in diagnosis and initial assessment, identifying active contrast extravasation (“blush”), pseudoaneurysms, or arteriovenous fistulas.
Interventional radiology has become indispensable in this setting. Transarterial embolization (TAE) is indicated in patients with evidence of active bleeding or vascular injury on CT, even in the absence of hemodynamic instability. Selective and superselective embolization techniques allow precise targeting, minimizing parenchymal loss while achieving effective hemostasis.
Complications such as bile leaks, bilomas, or delayed hemorrhage require vigilance. Many of these can also be managed percutaneously, reinforcing the central role of minimally invasive approaches.
Renal Trauma
Renal injuries account for approximately 1–5% of all trauma admissions, with most cases resulting from blunt trauma. Similar to liver injuries, the trend has shifted toward minimally invasive and conservative management, particularly for low- to moderate-grade injuries.
Multiphase-contrast enhanced CT imaging is again the diagnostic modality of choice, providing detailed information on parenchymal injury, urinary extravasation, and vascular involvement. The presence of active bleeding, expanding hematoma, or devascularization influences management decisions.
NOM is successful in the majority of cases, including many high-grade injuries. Interventional radiology plays a critical role in managing vascular complications such as pseudoaneurysms or ongoing hemorrhage through selective renal artery embolization. This approach preserves renal function while avoiding nephrectomy.
Urinary extravasation, particularly in high-grade injuries, may require intervention. Percutaneous drainage of urinomas and ureteral stenting are effective strategies that complement conservative management.
The evolution of trauma care has firmly established interventional radiology as a cornerstone of modern management. Rapid access to angiography suites and skilled operators is now considered essential in major trauma centers.
The advantages of embolization in the acute setting include:
- Precise and minimally invasive control of hemorrhage
- Organ preservation
- Reduced morbidity compared to surgery
However, appropriate patient selection is critical. Hemodynamically unstable patients who do not respond to resuscitation still require urgent surgical exploration. On the other hand, surgical packing or operative control may be ineffective or require extensive manipulations, as precise localization of hemorrhage is often not feasible, particularly in the presence of diffuse or multifocal bleeding. Moreover, during surgical exploration for hemorrhage control, the patient’s hemodynamic status may deteriorate following the release of tamponade achieved by prior abdominal packing. Thus, close collaboration between trauma surgeons, IRs and critical care teams is essential.
Emerging technologies, including advanced imaging, hybrid operating rooms, and navigation systems, are expected to further refine trauma care. Artificial intelligence may also enhance decision-making by improving risk stratification and possibly perform predictions of outcomes.
The increasing integration of interventional radiology into trauma algorithms and guidelines underscores the need for training and resource allocation, particularly in centers aiming to provide comprehensive trauma services.
In conclusion, the management of liver and kidney trauma exemplifies the broader evolution of trauma care toward less invasive, patient-centered strategies. With careful patient selection, robust imaging protocols and timely Interventional Radiology support on a 24/7 basis, outcomes continue to improve while preserving organ function and reducing complications.