Common iliac artery aneurysm occurs in 25% of patients with infrarenal aneurysms. The presence of a common iliac artery aneurysm not only serves as a second potential cause of aortic-related mortality, but may threaten the durability of EVAR by potentially limiting the distal landing zone. Early in the experience with EVAR, the technique of “Coil and Cover” the hypogastric was the hallmark. The discussion focused on the risk of hypogastric embolization and the techniques to reduce the risk of buttock claudication, sexual dysfunction, and pelvic ischemia by promoting collateral flow performing proximal embolization and staged embolization in patients requiring possible bilateral hypogastric sacrifice. Buttock claudication and sexual dysfunction occurred in greater than 50% of patients with unilateral hypogastric coverage.
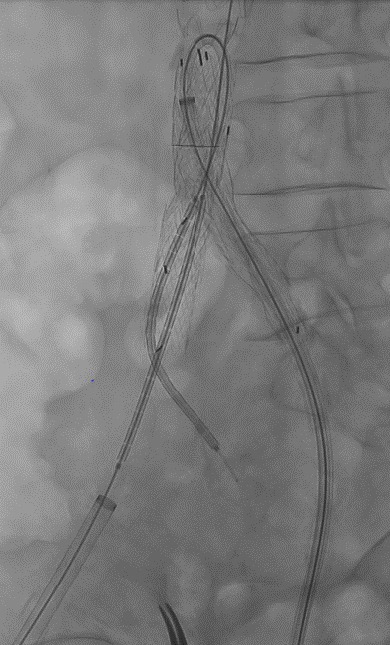
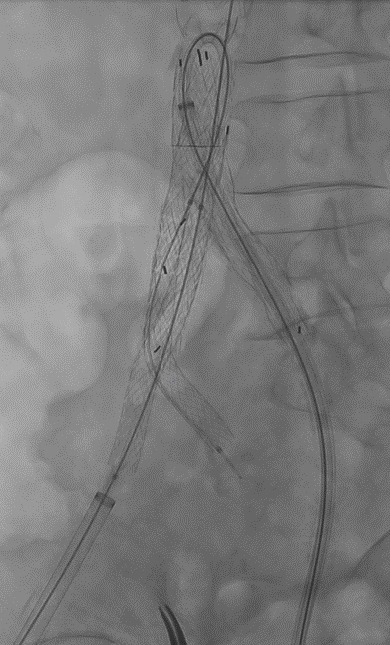
Over the last two decades, the understanding and techniques have evolved to provide several techniques to preserve hypogastric artery perfusion. Present techniques include: tube grafts (including retrograde hypogastric preservation) and bell bottom grafts into the distal common iliac artery; commercially available Iliac branch (IBE) devices; and double barrel graft techniques (parallel grafts).
How does one evaluate a patient and decide on possible treatment options?
Commercially available IBE devices are usually the first line devices. The data on the short-term technical results have now been augmented with longer term findings. The technical success rates are in the high 90% with the rate of early reinterventions at 1-4%. Understanding the anatomical recommendations for the IBE device is critical when deciding to proceed with an IBE repair. Considering the benefits and potential pitfalls of the techniques available for patients with less than ideal anatomy for an IBE device should guide the decision-making process when deciding double barrel techniques. The durability of bell bottom grafts is also important to consider. The Pelvic Registry from Italy has added much data on the durability of these repairs. The cost of these devices is also a factor that needs to be understood. The goal of creating a personalized endovascular solution for every patient and working to preserve hypogastric artery perfusion in the setting of common iliac aneurysms and proximal hypogastric aneurysms exist in 2024.